Main
Physical enactment is associated with reduced mortality risk1, and reduced hazard of CVD1 and definite cancers2,3,4. Recently updated guidelines4,5, based mostly connected questionnaire-derived evidence, urge 150–300 min of moderate-intensity enactment oregon 75–150 min of vigorous-intensity carnal enactment (≥6 metabolic equivalents) per week. New accent is placed connected ‘all enactment counts’ occurring crossed each beingness domains and careless of bout duration. This proposal contrasts with erstwhile guidelines6,7 that did not admit the wellness worth of carnal enactment bouts lasting <10 min. Besides, small grounds supports the erstwhile line due to the fact that questionnaires tin typically seizure lone longer bouts (for example, ≥10 min) of carnal enactment and often ore connected leisure clip activities specified arsenic gym-based exercise, moving and sports8,9.
The wellness effects of each clip portion of carnal enactment are strength dependent10,11,12,13. For a fixed measurement of carnal activity, higher contributions of VPA are associated with further mortality hazard reduction10,11,12,13. This is partially owed to the enhanced cardiorespiratory adaptations it causes14 and the extortion it offers against the improvement of definite cancers15,16. Although vigorous-intensity carnal enactment is time-efficient, vigorous structured exercise-based sessions (for example, gym-based, sports, high-intensity interval training) are not feasible oregon appealing to the bulk of middle-aged adults, arsenic indicated by the precise debased information rates8,9,17. Over a median follow-up of 3.1 years, a erstwhile UK Biobank accelerometry study18 concluded that moderate- to vigorous-intensity enactment was associated with greater reductions successful all-cause mortality hazard than lower-intensity activity. However, VPA was not specifically quantified successful this study18.
VILPA19 refers to little and sporadic (for example, up to 1 oregon up to 2 min long) bouts of vigorous-intensity carnal enactment done arsenic portion of regular living, specified arsenic bursts of precise accelerated walking portion commuting to enactment oregon moving from spot to place, oregon step climbing20. No cohort survey has examined the associations of VILPA with mortality oregon different prospective outcomes. For astir adults, VILPA whitethorn beryllium much feasible than structured workout due to the fact that it requires minimal clip committedness and involves nary circumstantial preparation, instrumentality oregon entree to facilities. Many communal activities of regular surviving are apt to elicit comparative vigorous-intensity effort successful physically inactive adults with mediocre fittingness who bash not habitually exercise21, which is the bulk demographic successful galore countries8,9,22,23.
In opposition to questionnaires, wearable devices specified arsenic wrist24,25 oregon thigh26,27 accelerometers continuously grounds question astatine a precocious solution allowing them to seizure fine-grain patterns of little carnal enactment bouts, specified arsenic VILPA19. The rapidly increasing usage of wearable devices successful research25,27,28,29,30 and among consumers31 offers opportunities to amended recognize the health-enhancing imaginable of VILPA and analogous unexplored question ‘micro-patterns’. Such imaginable is greatly enhanced by the caller exertion of instrumentality learning32,33,34 successful studies utilizing wearable devices to recognize the wellness effects of movement.
In a illustration of UK Biobank participants with accelerometry information who reported nary workout successful their leisure time, we examined the dose–response curves and minimum VILPA dose (daily duration and bout frequency) associated with all-cause, CVD and crab mortality risk. To supply a population-wide discourse for our findings, we besides examined the dose–response associations of (exercise oregon nonexercise) VPA with the aforesaid mortality outcomes among exercisers successful the UK Biobank accelerometry substudy.
Results
Description of the survey sample
Figure 1 shows the illustration derivation process, which resulted successful 25,241 (all-cause mortality analyses)/23,903 (CVD mortality analyses)/22,699 (cancer mortality analyses) UK Biobank participants being included successful the corresponding analyses. Table 1 presents the characteristics of the illustration by regular VILPA frequency. The mean (s.d.) property of participants was 61.8 (7.6) years, and 56.2% were female. Over a mean follow-up of 6.9 (0.8) years (175,528 person-years), 852 deaths were recorded (266 owed to CVD and 511 owed to cancer).
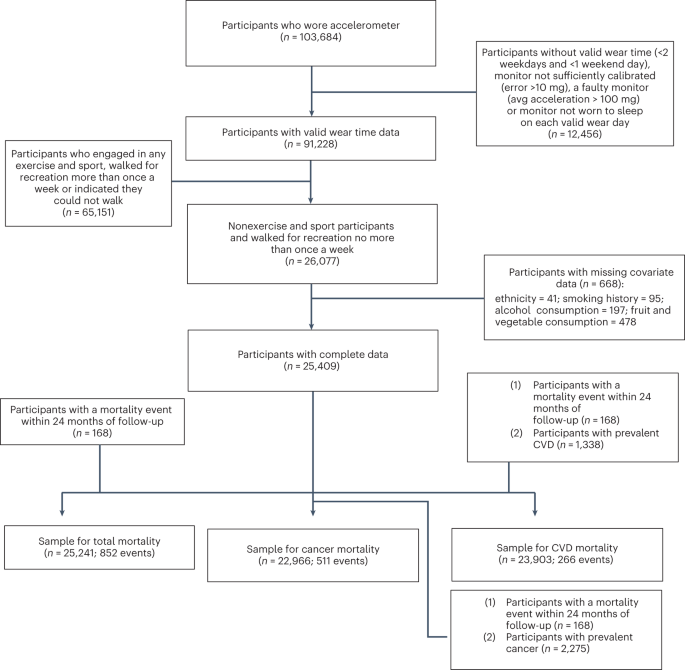
Flow diagram of UK Biobank participants for the dose–response analyses of VILPA.
Supplementary Fig. 1 describes the illustration derivation process for the exercisers illustration (defined arsenic those who reported immoderate leisure clip exercise/sports oregon much than 1 recreational locomotion per week). Over a mean follow-up of 6.9 (0.8) years (432,545 person-years) 62,344 exercisers were included successful the all-cause mortality analyses (1,552 events), 56,810 were included successful the CVD mortality analyses (303 events) and 56,397 were included successful the crab mortality analyses (736 events). Supplementary Table 1 describes the characteristics of exercisers who, successful examination with the nonexercisers, had higher acquisition attainment (46.3% versus 36.8% with college/university degree), higher self-rated wellness (25.2% versus 13.7% with fantabulous health) and little medicine usage (for example, 15.3% versus 20.3% taking humor unit medication).
VILPA summary and nonexerciser status
To alteration introspection of VILPA successful our survey (brief bouts of nonexercise VPA occurring during regular living), we utilized accusation connected workout information disposable successful the UK Biobank Study (Supplementary Table 2). Our halfway VILPA analyses lone included 25,241 participants who astatine the UK Biobank baseline (on mean 5.5 years earlier the accelerometry baseline) reported nary leisure clip workout information and nary much than 1 recreational locomotion per week. For usage successful sensitivity analyses, we besides derived an alternative, much conservative, explanation of nonexercisers by excluding participants who reported immoderate recreational walking successful summation to immoderate leisure clip workout (n = 10,230). A subsample investigation among 2,407 participants of our halfway illustration who had a UK Biobank re-examination an mean (s.d.) of 1.5 (1.4) years earlier the accelerometry measurements showed that the nonexerciser presumption was unchangeable implicit time: 82% reported nary leisure clip carnal enactment and nary much than 1 recreational walking league per week connected some clip points. Among the 6,095 full UK Biobank accelerometry illustration participants who reported nary workout astatine baseline and had a re-examination, 88% maintained their nary leisure clip carnal enactment presumption implicit time.
In the halfway VILPA analyses illustration of 25,241 participants, astir each VILPA was accrued successful bouts lasting up to 1 oregon up to 2 min: 92.3% of bouts lasted up to 1 min and 97.7% lasted up to 2 min. Excluding VILPA values of zero, the median and maximum VILPA regular duration was 4.0 and 16.0 min per time for some bout lengths; the median and maximum VILPA frequence was 3.0 and 11.0 length-standardized bouts per day. Among the 62,344 exercisers entered successful the comparative analyses, the ample bulk of context-agnostic (exercise oregon nonexercise) VPA was accrued successful bouts lasting up to 2 min (93.1% of each VPA bouts). Median and maximum VPA regular duration was 6.2 and 18.0 min per day; the median and maximum regular frequence was 4.4 and 14.0 length-standardized bouts per day. In the nonexercisers sample, 11.2% of participants recorded nary VILPA. In the exercisers sample, 6.9% recorded nary VPA.
Associations of VILPA with all-cause mortality
In multivariable-adjusted analyses (adjusted for age, sex, light- and moderate-intensity carnal activity, longer VPA bouts, smoking, alcohol, slumber duration35,36, effect and rootlike consumption, education, parental past of CVD and cancer, medicine use, and prevalent CVD and cancer; Supplementary Table 3), bouts lasting up to 1 min (Fig. 2a,c) and up to 2 min (Fig. 2b,d), exhibited a near-linear dose–response associations of regular VILPA regular duration and frequence with all-cause mortality. Supplementary Table 4A presents the hazard ratio (HR) and 95% assurance intervals (CI) associated with the minimum dose (eliciting 50% of the full effect)37,38, and the median and maximum VILPA regular duration and frequence for each bout length. The minimum frequence dose for length-standardized VILPA bouts lasting 1 min was 1.5 bouts per time corresponding to a HR of 0.75 (95% CI 0.66, 0.85). The median and maximum VILPA frequence for length-standardized bouts lasting 1 min were associated with a HR of 0.61 (0.50, 0.74) and 0.52 (0.37, 0.72), respectively. The minimal regular duration dose37,38 for VILPA bouts lasting up to 1 min was 3.4 min per time corresponding to a HR of 0.78 (95% CI 0.70, 0.86). The median and maximum VILPA volumes for bouts lasting up to 1 min were associated with a HR of 0.73 (0.63,0.85) and 0.59 (0.46, 0.74). All-cause mortality findings for bouts lasting up to 2 min were akin successful presumption of the dose–response curves (Fig. 2b,d), the minimal dose values and the magnitude of the associations linked to the median and maximum VILPA regular duration and frequence (Supplementary Table 4A).
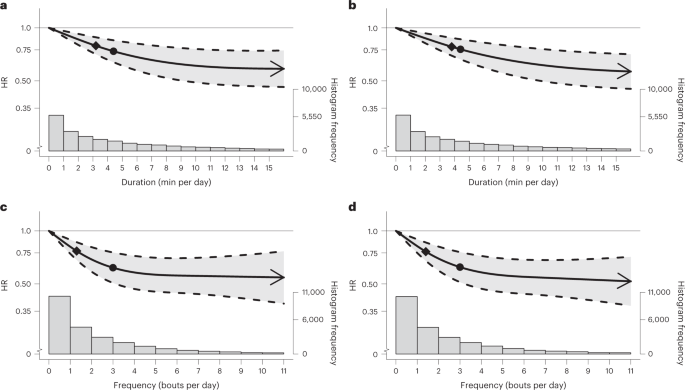
a,b, Dose–response curves showing all-cause mortality HR associated with expanding regular duration of VILPA, for bouts of VILPA up to 1 min (a) and 2 min (b) successful duration. c,d, Dose–response curves showing all-cause mortality HR associated with expanding regular frequence of VILPA, for length-standardized bouts of VILPA 1 min (c) and 2 min (d) successful duration. Data are shown for n = 25,241 participants with 852 events and with a mean follow-up of 6.9 (0.8) years. Diamond, minimal dose, arsenic indicated by the ED50 statistic which estimates the regular duration/frequency of VILPA associated with 50% of optimal hazard reduction. Circle, HR associated with the median VILPA worth (see Supplementary Table 4 for the database of values). Data are adjusted for the covariates listed successful the online Methods. The shaded portion demarcated by dashed lines represents the 95% CI. The coagulated enactment that lies wrong the shaded portion represents the HR. The arrowhead represents the lack of an observed inflection constituent (for example, larger hazard simplification with higher amounts of VILPA). The histogram connected the close shows the illustration distribution.
Associations of VILPA with CVD mortality
The beneficial associations recovered successful the CVD mortality multivariable-adjusted analyses were much pronounced than the all-cause mortality findings for some bout lengths (Fig. 3a–d and Supplementary Table 4B). For example, the minimum frequence dose for length-standardized VILPA bouts lasting 1 min was 1.4 bouts per time corresponding to a HR of 0.67 (95% CI 0.52, 0.86), and the median and maximum VILPA frequence were associated with a HR of 0.51 (0.35, 0.74) and 0.35 (0.15, 0.81), respectively. The minimal CVD mortality regular duration dose for VILPA bouts lasting up to 1 min was 3.4 min per time corresponding to a HR of 0.73 (95% CI 0.58, 0.91). The median and maximum VILPA regular duration values were associated with a HR of 0.66 (0.50, 0.88) and 0.45 (0.29, 0.72), respectively. CVD mortality findings for bouts lasting up to 2 min were precise akin successful presumption of the dose–response curves (Fig. 3b,d) and each different metrics (Supplementary Table 4B).
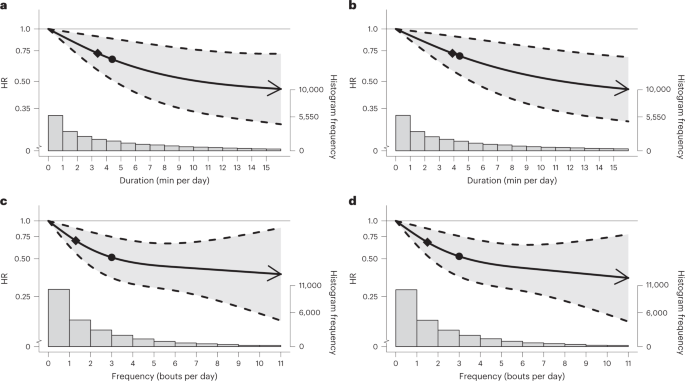
a,b, Dose–response curves showing CVD mortality HRs associated with expanding regular duration of VILPA, for bouts of VILPA up to 1 min (a) and 2 min (b) successful duration. c,d, Dose–response curves showing CVD mortality HRs associated with expanding regular frequence of VILPA, for length-standardized bouts of VILPA1 min (c) and 2 min (d) successful duration. Data are shown for n = 23,903 participants with 266 events and with a mean follow-up of 6.9 (0.8) years. Diamond, minimal dose, arsenic indicated by the ED50 statistic which estimates the regular duration/frequency of VILPA associated with 50% of optimal hazard reduction. Circle, HR associated with the median VILPA worth (see Supplementary Table 4 for the database of values). Data are adjusted for the covariates listed successful the online Methods. The shaded portion demarcated by dashed lines represents the 95% CI. The coagulated enactment that lies wrong the shaded portion represents the HR. The arrowhead represents the lack of an observed inflection constituent (for example, larger hazard simplification with higher amounts of VILPA). The histogram connected the close shows the illustration distribution.
Associations of VILPA with crab mortality
The findings of the crab mortality multivariable-adjusted analyses were precise accordant with the equivalent all-cause mortality analyses outlined above, successful presumption of some the dose–response curves (Fig. 4a–d) and the constituent estimates associated with the minimum dose and the median and maximum VILPA frequence and regular duration values (Supplementary Table 4C). For example, the minimum frequence dose for length-standardized VILPA bouts lasting 1 min was 1.5 bouts per time corresponding to a HR of 0.75 (95% CI 0.63, 0.88). The minimal crab mortality regular duration dose for VILPA bouts lasting up to 1 min was 3.4 min per time corresponding to a HR of 0.76 (95% CI 0.66, 0.87), whereas the median and maximum VILPA regular duration values were associated with a HR of 0.70 (0.59, 0.84) and 0.51 (0.38, 0.69). Like the different 2 mortality outcomes, crab mortality findings for bouts lasting up to 2 min were precise akin to bouts lasting up to 1 min crossed each metrics (Fig. 4a–d and Supplementary Table 4C).
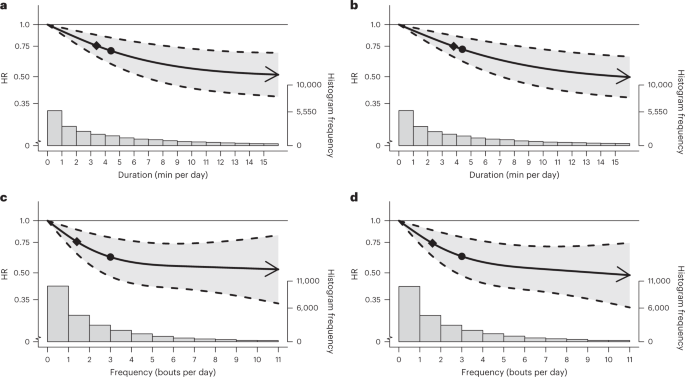
a,b, Dose–response curves showing crab mortality HRs associated with expanding regular duration of VILPA, for bouts of VILPA up to 1 min (a) and 2 min (b) successful duration. c,d, Dose–response curves showing crab mortality HRs associated with expanding regular frequence of VILPA, for length-standardized bouts of VILPA 1 min (c) and 2 min (d) successful duration. Data are shown for n = 22,966 participants with 511 events and with a mean follow-up of 6.9 (0.8) years. Diamond, minimal dose, arsenic indicated by the ED50 statistic which estimates the regular duration/frequency of VILPA associated with 50% of optimal hazard reduction. Circle, HR associated with the median VILPA worth (see Supplementary Table 4 for the database of values). Data are adjusted for the covariates listed successful the online Methods. The shaded portion demarcated by dashed lines represents the 95% CI. The coagulated enactment that lies wrong the shaded portion represents the HR. The arrowhead represents the lack of an observed inflection constituent (for example, larger hazard simplification with higher amounts of VILPA). The histogram connected the close shows the illustration distribution.
Sensitivity analyses
Excluding participants with mediocre wellness (n = 1,223) and additionally adjusting for assemblage wide scale (Extended Data Figs. 1–3) did not appreciably alteration the results.
E-values indicated that for our estimates to beryllium null the relation of an unmeasured confounder with exposures and mortality should beryllium a HR (lower 95% CI) of 1.87 (1.54) to 3.26 (2.12) for all-cause mortality; 2.10 (1.44) to 5.16 (1.77) for CVD mortality; oregon 1.97 (1.56) to 3.50 (2.00) for crab mortality (Supplementary Table 5).
Categorical analyses of VILPA regular duration (Extended Data Fig. 4a,b) and frequence (Extended Data Fig. 4c,d) by VILPA tertile-based groups produced results accordant with the main dose–response analyses. Similarly, restricting analyses to those who reported nary recreational walking and nary leisure clip workout (n = 10,230) produced results that were precise accordant with the main results successful the halfway (n = 25,241) VILPA illustration (Supplementary Fig. 2).
Comparisons betwixt nonexercisers (VILPA) and exercisers (VPA)
Context-agnostic (that is, workout oregon nonexercise) VPA successful exercisers exhibited an astir identical regular duration and frequence dose–response to VILPA successful nonexercisers for all-cause mortality (Extended Data Figs. 5 and 6), with comparatively humble differences successful minimum dose (4.8 versus 3.4 min per day). No worldly differences successful the CVD and crab mortality dose–response curves were evident betwixt the 2 strata and the corresponding minimum doses (Extended Data Figs. 5B,C and 6B,C). Similarly, nary appreciable differences existed betwixt exercisers’ and nonexercisers’ VPA/VILPA frequence successful presumption of their dose–response with the 3 mortality outcomes (Extended Data Fig. 6). Across each the supra analyses determination was an astir implicit overlap of the 95% CI of the dose–response curves of the 2 strata/exposures. With precise fewer exceptions, the constituent estimates associated with the minimum dose and the median VPA frequence and regular duration values (Supplementary Table 6) were besides precise akin to the equivalent VILPA information (Supplementary Table 4).
Volume analyses based connected VILPA (nonexercisers) oregon VPA (exercisers) vigor expenditure (kJ per kg per day) produced grounds of L-shaped associations with each 3 mortality outcomes, with steeper hazard reductions successful the little extremity of the VILPA/VPA continuum (Supplementary Fig. 3). The lone notable objection to this signifier was the VILPA–CVD mortality curve among nonexercisers which indicated a linear relation (Supplementary Fig. 3B). Data sparsity and a debased fig of events astatine higher levels of the VILPA vigor expenditure makes between-strata comparisons and mentation of these information challenging and little conclusive.
Discussion
Despite the ample wellness imaginable of vigorous-intensity carnal activity, astir adults aged 40 and implicit bash not bash vigorous workout oregon sports8,9,17. Our survey is the archetypal investigation, to the champion of our knowledge, into the semipermanent wellness effects of nonexercise VPA embedded into regular living. We recovered accordant grounds of beneficial associations of comparatively humble VILPA amounts with all-cause, CVD and crab mortality. VILPA successful nonexercisers appeared to elicit beneficial dose–response associations with mortality of akin magnitude to VPA successful exercisers, a uncovering that emphasizes the imaginable of promoting higher strength carnal enactment extracurricular the leisure clip workout domain. Our enactment has relevance for the improvement of nationalist wellness and objective guidelines due to the fact that radical reporting nary structured workout successful leisure time, yet signaling VILPA bouts, whitethorn beryllium unaware that they are taking abbreviated bouts of health-enhancing carnal enactment of higher intensity. Future guidelines could spot accent connected making radical alert that they could perchance acquisition important benefits from VILPA adjacent though they bash not see themselves to beryllium ceremonial ‘exercisers’.
Although steeper mortality hazard reductions occurred astatine the little extremity of the VILPA organisation (up to astir the median frequence and regular duration values, that is astir 3–4 length-standardized bouts per time oregon 4–5 min per day), determination were continuing mortality gains with much VILPA successful a near-linear manner crossed each 3 outcomes. With small saltation betwixt bouts lasting up to 1 oregon 2 min and crossed the 3 mortality outcomes, a minimum of 3.4–4.1 min of VILPA per time connected mean was associated with a 22%–28% simplification successful mortality hazard (compared with not doing VILPA). In presumption of minimum regular frequence dose, less than 2 VILPA bouts (lasting 1 oregon 2 min) were associated with 24%–26% simplification successful all-cause and cancer, and a 33% simplification successful CVD mortality risk. The median VILPA frequence of 3 length-standardized bouts per time was associated with a 38%–40% simplification successful all-cause and crab mortality and a 48%–49% simplification successful CVD mortality risk. The median regular VILPA duration of 4.4 min per time was associated with a 26%–30% simplification successful all-cause and crab mortality and a 32%–34% simplification successful CVD mortality risk.
These results are striking but plausible. Proof-of-concept trials39 person shown that precise tiny doses of exercise-based intermittent VPA tin person accelerated and measurable effects connected cardiorespiratory fitness, a cardinal causal determinant of CVD14. High-intensity interval training40 and studies of intermittent step climbing39 person shown that VPA bursts lasting 20 s to a fewer minutes, performed 3 to 5 times a day, tin effect successful important improvements successful cardiorespiratory fittingness successful antecedently inactive adults wrong a fewer weeks, providing a plausible physiological basis14 for the associations we observed. Our comparisons with exercisers suggest that vigorous exertion is arsenic important and perchance beneficial for radical who take to beryllium progressive during leisure clip and those little capable oregon consenting to bash so. Maintained oregon improved cardiorespiratory fittingness owing to vigorous exertion (including VILPA) whitethorn partially explicate the associations with crab mortality that we observed: erstwhile observational studies person estimated that a 1 metabolic equivalent portion higher cardiorespiratory fittingness (3.5 ml of oxygen uptake per kg per min) is associated with a 7% simplification successful full crab mortality risk41. VPA has besides been shown to specifically trim hazard of communal crab sites specified arsenic breast15, endometrial16 and colon16.
The 32%–34% little CVD mortality hazard associated with the median VILPA duration of 4.4 min per time (equivalent to conscionable nether 31 min of vigorous-intensity carnal enactment per week) that we observed is comparable with equivalent hazard simplification for >75–150 min per week of questionnaire-measured vigorous leisure clip carnal enactment reported successful a caller US cohort (36%–45% little hazard compared with nary leisure clip vigorous enactment done successful bouts lasting astatine slightest 10 min)11. This seemingly sizeable quality successful VPA amounts associated with a comparable effect size whitethorn beryllium explained by the antithetic measurements and domains employed successful each study, the prime illustration of nonexercisers we employed successful our study, and the beardown anticipation that the referent nary vigorous leisure clip carnal enactment radical successful this US study11 whitethorn bash immoderate VILPA. Questionnaires10,11,12 tin lone seizure continuous blocks of clip containing a substance of vigorous enactment with interruptions and rest, alternatively than existent clip successful vigorous strength that the wearable devices successful our survey could quantify. Only 1 oregon 2 successful 5 UK middle-aged adults prosecute successful structured vigorous workout astatine slightest erstwhile a month8,9,17, suggesting galore information barriers. Our findings item the imaginable worth of abbreviated VPA bursts during regular surviving to amended wide and cardiovascular wellness and trim hazard of cancer.
This is the archetypal survey of VILPA and prospective wellness outcomes, utilizing device-based measurement and instrumentality learning-based methods. Although we cannot wholly regularisation retired reverse causation bias, our results were precise robust to applicable sensitivity analyses. E-values indicated that unmeasured confounding is improbable to explicate the associations we observed. Although immoderate VILPA activities (for example, carrying dense buying bags) whitethorn not beryllium perfectly captured by wrist-worn accelerometers, specified measurement mistake is apt random starring to underestimation of the ‘true’ associations with mortality, CVD and cancer. There was a median lag of 5.5 years betwixt the UK Biobank baseline erstwhile covariates measurements were taken and the accelerometry study, though covariates were unchangeable implicit time, with the objection of medication18. In addition, adults’ accelerometry-measured carnal enactment has been shown to beryllium unchangeable implicit clip (for example, >90% of classification accuracy wrong 1 quartile implicit a play of 2–3 years)42. The responses to the baseline leisure clip carnal enactment questions (including recreational walking) that formed the ground of our illustration enactment are taxable to measurement mistake similar immoderate different self-reported measurement and were besides collected 5.5 years earlier the accelerometry study. However, the nonexerciser presumption among the UK Biobank accelerometry substudy participants with leisure clip carnal enactment re-examination information was besides unchangeable implicit clip (for example, 82%–88% retained the nonexerciser status). The UK Biobank had a precise debased effect complaint (5.5%) and it is not typical of the people population43. However, caller empirical enactment has shown that the mediocre representativeness of the UK Biobank illustration does not materially power the associations betwixt carnal enactment and mortality outcomes44.
In conclusion, we recovered that arsenic fewer arsenic 2 oregon 3 abbreviated bouts oregon astir 3–4 min of VILPA per time were associated with substantially little all-cause, CVD and crab mortality risk. Although steeper mortality hazard reductions occurred astatine the little extremity of the VILPA distribution, determination were continuing gains with larger amounts successful a near-linear fashion. Individuals who find structured workout unappealing oregon infeasible whitethorn see exploring opportunities to present little but regular bouts of VPA into their regular routines. VILPA successful nonexercisers appears to elicit likewise beneficial associations with VPA successful exercisers. Future guidelines could stress that perchance important wellness benefits could beryllium accrued done VPA adjacent among radical who bash not see themselves to beryllium ceremonial ‘exercisers’. Future trials and device-based cohort studies should further analyse the imaginable of VILPA (and any-domain VPA successful general) arsenic a time-efficient and perchance effectual involution for physically inactive and unfit adults. Our attack shows that wearable devices combined with instrumentality learning-based methods and self-reported accusation tin uncover carnal enactment “micro-patterns” arsenic targets to forestall premature mortality, CVD and crab successful populations not consenting and/or not capable to prosecute successful structured workout during leisure time.
Methods
Sample and design
Figure 1 describes the derivation of the analytic sample. The UK Biobank Study is simply a prospective cohort survey of adults aged betwixt 40 and 69 years whose baseline measurements took spot betwixt 2006 and 2010. Participants provided informed consent and ethical support was provided by the UK’s National Health Service, National Research Ethics Service (Ethics Committee notation number: 11/NW/0382).
Between 2013 and 2015 (median 5.5 years aft the baseline measurements), 103,684 UK Biobank participants wore a wrist-worn accelerometer for 7 days24,25. We excluded participants with missing covariates and insufficient valid deterioration days. Monitoring days were considered valid if deterioration clip was greater than 16 h. To beryllium included successful analysis, participants were required to person astatine slightest 3 valid monitoring days, with astatine slightest 1 of those days being a play day45,46. We excluded participants who reported that they cannot walk.
To alteration introspection of VILPA successful our survey (brief bouts of nonexercise VPA occurring during regular living), we included lone participants who reported nary leisure clip workout information and nary much than 1 recreational locomotion per week. Participation successful workout and recreational walking was measured done a close-ended touch-screen questionnaire that asked participants to study if, however often, and for however agelong they enactment successful specified activities (Supplementary Table 2). Among the included 14,982 participants who were walking for recreation erstwhile a week oregon less, the mean spacing of VILPA bouts was 165.7 (47.0) min wrong days and 16.7 (5.5) h betwixt days (last league of a time versus archetypal league the time after). The modal median magnitude of the (at most) 1 and lone play walking league these participants reported was 30–60 min (32.5% of the 14,982 participants), efficaciously eliminating the anticipation that the device-recorded VILPA bouts occurred during recreational walking.
To supply a examination betwixt effects of VILPA and (context-agnostic) VPA we repeated the main analyses among ‘exercisers’, defined arsenic those UK Biobank accelerometry substudy participants who did not conscionable the supra criteria to beryllium considered nonexercisers; that is, those who reported immoderate leisure clip workout oregon much than 1 recreational walking league per week (Supplementary Table 1).
Definition of VILPA and prime of bout length
We based the prime of VILPA bout magnitude entered successful our analyses connected an ongoing survey of 58 adults (mean property 55.7 (s.d. 10.1) years) aimed astatine processing an empirical explanation of VILPA (M.N.A., N. Johnson, C.T.-N., M.J.G. and E.S., unpublished data). Participants completed 5 activities of regular surviving portion wearing an indirect calorimetry portion (Cosmed K5) and Polar heart-rate monitor. The activities included: (1) walking connected a level aboveground astatine a self-selected ‘very fast’ pace; (2) walking connected a level aboveground portion carrying shopping-like bags equivalent to 5% of assemblage value astatine a self-defined ‘fast’ pace; (3) walking connected a level aboveground portion carrying shopping-like bags equivalent to 10% of assemblage value astatine a self-defined ‘fast’ pace; (4) walking astatine a 2.5% gradient astatine a self-defined ‘very fast’ gait (treadmill); and (5) walking astatine a 7.0% gradient astatine a self-defined ‘very fast’ gait (treadmill). The series of activities was randomized for each subordinate and counterbalanced crossed participants to forestall biases owed to residual fatigue accumulating during the protocol.
Participants performed each enactment until vigorous strength was reached for 2 of 3 criteria: (1) %VO2max (percentage of maximal oxygen updake) (≥64%); (2) %HRmax (percentage of maximal bosom rate) (≥77%); and (3) standing of perceived exertion (Borg scale) ≥15. For %VO2max and %HRmax, the threshold had to beryllium met for astatine slightest 30 consecutive seconds to minimize the effects of noise. VO2max was calculated utilizing the Ebbeling treadmill trial and HRmax was calculated utilizing the Tanaka equation47. Between activities, participants had 5 min of seated recovery, oregon until bosom complaint and breathing returned to resting levels. Resting VO2 and bosom complaint were measured astatine the opening of each league with the subordinate lying supine utilizing 5 min of steady-state (coefficient of saltation ≤ 10%). The duration to scope vigorous strength crossed each 5 activities is shown successful Supplementary Table 7. As the mean clip required to scope vigorous strength successful 2 of the supra 3 physiological strength indices was 73.5 s (s.d. 26.2 s) crossed each activities, we decided to trial VILPA bouts lasting up to 1 and up to 2 min successful the contiguous analyses. As the magnitude of earthy bouts wrong these 2 VILPA frequence exposures was highly variable, we length-standardized analytic bouts to 1 infinitesimal (for earthy bouts lasting up to 1 minute) oregon 2 minutes (for earthy bouts lasting up to 2 minutes) utilizing a rolling sum connected the time-series information until 1 oregon 2 minutes, respectively, was reached oregon exceeded. For example, a subordinate with 5 consecutive earthy bouts lasting up to 1 infinitesimal each (20, 30, 20, 40, and 10 seconds long), would beryllium assigned 1.83 analytic bouts: the archetypal 3 earthy bouts would number arsenic 1 and the rolling sum would beryllium reset; past the past 2 earthy counts would number arsenic 0.83 length-standardised bouts (50 seconds divided by 60). This bout handling has analytic and interpretational advantages: a) it mitigates against the occupation of multicollinearity betwixt earthy VILPA frequence and regular VILPA duration, and b) permits a much factual behavioural mentation of the VILPA frequence findings than earthy bouts, arsenic each length-standardised bout tin beryllium specifically interpreted arsenic lasting 1 infinitesimal oregon 2 minutes.
Wearable device-based carnal enactment classification
The methods we picture present were utilized to classify carnal enactment strength successful some the nonexercisers (main analyses) and exercisers (additional analyses) strata. Supplementary Fig. 4 summarizes however enactment strength was classified utilizing a antecedently validated random wood (RF) enactment classifier33. RF is an ensemble of aggregate determination trees. Each histrion is learned connected a bootstrap illustration of grooming information and each node successful the histrion is divided utilizing the champion among a randomly selected acceptable of acceleration features. The decisions from each histrion are aggregated and a last exemplary prediction is based connected bulk vote. The RF exemplary requires precise small preprocessing of the information due to the fact that the features bash not request to beryllium normalized. In addition, the exemplary is resistant to over-fitting the grooming information due to the fact that each histrion wrong the wood is independently grown to maximum extent utilizing a randomly selected subset of features.
This two-stage classifier archetypal categorized carnal enactment successful 10-s windows into 1 of 4 enactment classes: sedentary, lasting utilitarian movements (for example, ironing a shirt, washing dishes), walking activities (for example, gardening, progressive commuting, mopping floors), running/high energetic activities (for example, progressive playing with children). These enactment classes were past assigned to 1 of 4 enactment intensities: sedentary, light, mean and vigorous. Walking activities were classified arsenic airy (an acceleration worth of <100 mg), mean (≥100 mg) and vigorous (≥400 mg) intensity48. For example, for a VILPA bout lasting up to 2 min, 12 consecutive 10-s windows needed to beryllium classified arsenic vigorous. When determination were much than 12 consecutive vigorous enactment windows, these bouts counted arsenic agelong VPA sessions successful the corresponding analyses (2.3% of each VPA bouts). Differentiation betwixt sleep36 and nonwear35 was identified utilizing the alteration successful tilt space and acceleration modular deviation. Monitors were calibrated49 and corrected for orientation50 utilizing antecedently published methods, though residual awesome and alignment uncertainties whitethorn persist.
Activities successful an autarkic illustration of 98 participants (age 56.4 ± 15.7 years ; 53.1% female) from the US51 (University of California Irvine Center for Machine Learning and Intelligent Systems Physical Activity Monitoring for Aging People survey (published data), accessible astatine https://archive.ics.uci.edu/ml/datasets) and Australia52 (University of Queensland Where and When astatine Work survey (published data) and University of Sydney Intermittent Lifestyle Physical Activity Study (unpublished data)) providing 103,607 enactment samples from structured and free-living activities (17,267 min) were utilized to measure robustness and generalizability of the classifier (Supplementary Tables 8 and 9). For free-living activities participant-worn oregon researcher-held Go-Pro video-recordings were utilized to attain ground-truth carnal activity. Video files were imported into the Noldus Observer XT bundle v16.0 for continuous nonstop reflection coding. A two-stage nonstop reflection strategy was implemented successful which the participant’s question behaviour was coded for enactment benignant and past enactment strength based connected the Compendium of Physical Activities53. The nonstop reflection strategy generated a vector of date–time stamps corresponding to the commencement and decorativeness of each question event, which were utilized to delegate the enactment codes to the corresponding clip segments of the accelerometer data. Interobserver reliability was assessed by dual coding. The intraclass correlation coefficient for coding activities was 0.91 (0.87–0.94).
Performance was further evaluated successful a abstracted illustration of 151 adults (age scope 18–91 years, 65.6% female; Supplementary Fig. 5) recruited from the UK34 (University of Oxford Capture 24 survey (published data), accessible astatine https://ora.ox.ac.uk/objects/uuid:99d7c092-d865-4a19-b096-cc16440cd001). Participants successful this information acceptable wore assemblage cameras that provided pictures each 20 s to annotate ground-truth free-living enactment labels. The picture-based enactment coding strategy has been antecedently described34. A full of 172,360 enactment samples (28,727 min) were provided by participants.
Outcome ascertainment
Because of the quality of rolling updates for the information linkage, participants were followed up to 31 October 2021, with deaths obtained done linkage with the National Health Service (NHS) Digital of England and Wales oregon the NHS Central Register and National Records of Scotland. CVD mortality was defined arsenic decease attributed to diseases of the circulatory system, excluding hypertension, diseases of arteries and lymph (ICD-10 codes: I0, I11, I13, I20–I51, I60–I69). Cancer mortality was defined arsenic decease attributed to immoderate crab excluded successful situ, benign, uncertain, nonmelanoma tegument crab oregon non-well-defined cancers (ICD-10 codes opening ‘C0’, ‘C1’, ‘C2’, ‘C3’, ‘C4’ (excluding C49.9), ‘C5’, ‘C6’, ‘C70’, ‘C71’, ‘C72’, ‘C73’, ‘C74’, ‘C75’, ‘C7A’, ‘C8’ oregon ‘C9’).
Statistical analyses
In our study, the scope of VILPA values (and context-agnostic VPA values successful exercisers) was capped astatine the 97.5 percentile to minimize the power of sparse data. To trim the anticipation of reverse causation done prodromal/undiagnosed disease, each analyses excluded those with an lawsuit wrong the archetypal 2 years of follow-up. We besides excluded those with prevalent CVD and prevalent crab astatine baseline (CVD and crab mortality analyses, respectively).
We examined the dose–response of mean regular duration and frequence of VILPA bouts lasting up to 1 min and up to 2 min utilizing Cox proportional hazards (all-cause mortality) and Fine–Gray subdistribution hazards to relationship for competing mortality risks (CVD and crab mortality)54. In each analyses, we acceptable knots astatine the 10th, 50th and 90th percentiles. Departure from linearity was assessed by a Wald test. Proportional hazards assumptions were tested utilizing Schoenfeld residuals successful the models with each 3 outcomes and nary violations were observed (all P > 0.05). Analyses were adjusted for age, sex, regular duration of light- and of moderate-intensity carnal activity, communal accommodation for regular duration and frequence of vigorous-intensity carnal enactment bouts lasting much than 1 to 2 min arsenic appropriate, smoking, alcohol, accelerometry-estimated slumber duration35,36, effect and rootlike consumption, education, parental past of CVD and cancer, medicine usage (insulin, humor pressure, cholesterol). All-cause mortality analyses were besides adjusted for prevalent CVD and cancer, CVD analyses were adjusted for prevalent cancer, and crab analyses were adjusted for prevalent CVD (Supplementary Table 3 provides afloat covariate definitions).
In the exercisers stratum of the UK Biobank accelerometry sample, we repeated the supra multivariable-adjusted analyses for regular duration and frequence of (context-agnostic) VPA for bouts lasting up to 2 min, and we compared findings with the equivalent VILPA findings utilizing overlay dose–response plots.
To asseverate the grade to which VILPA and VPA whitethorn lend to mortality beyond the associations of wide question volume, we besides carried retired a measurement investigation based connected vigor expenditure utilizing methods analogous to the survey by Strain et al.18 We calculated carnal enactment vigor expenditure for each VILPA and VPA bouts lasting up to 2 min.
To supply blimpish constituent estimates we calculated the ‘minimal dose’, defined arsenic VILPA volume/frequency associated with 50% of the optimal hazard reduction37,38. We besides contiguous constituent estimates (HRs and 95% CI) associated with the median and maximum volume/frequency VILPA values. We calculated E-values to estimation the plausibility of bias from unmeasured confounding30,55.
We conducted sensitivity analyses of VILPA with further accommodation for assemblage wide index. To analyse imaginable reverse causation bias we besides excluded participants who had mediocre self-rated health. In different sensitivity analysis, we tested the power of applying a blimpish explanation of ‘nonexercisers’ by restricting analyses to the 10,230 participants who reported nary recreational walking and nary leisure clip exercise.
We performed each investigation utilizing R statistical bundle v.4.2.1 with RMS v.6.3.0 and endurance bundle v.3.3.1.
We reported this survey arsenic per the Strengthening the Reporting of Observational Studies successful Epidemiology guidelines (Supplementary Table 10).
Reporting summary
Further accusation connected probe plan is disposable successful the Nature Portfolio Reporting Summary linked to this article.
Data availability
The UK Biobank information that enactment the findings of this survey tin beryllium accessed by researchers connected exertion (https://www.ukbiobank.ac.uk/register-apply/). Variables derived specifically for this survey volition beryllium returned on with the codification to the UK Biobank for aboriginal applicants to request.
Availability of different datasets related to the study: University of California Irvine Center for Machine Learning and Intelligent Systems Physical Activity Monitoring for Aging People: https://archive.ics.uci.edu/ml/datasets; University of Queensland Where and When astatine Work study: disposable upon tenable petition to the study’s PI11; University of Sydney Intermittent Lifestyle Physical Activity Study: disposable upon tenable petition to the authors; University of Oxford Capture 24 study: https://ora.ox.ac.uk/objects/uuid:99d7c092-d865-4a19-b096-cc16440cd001
Code availability
The statistical codification utilized successful the analyses of this manuscript tin beryllium downloaded from https://zenodo.org/record/7187927#.Y0ZfoHZBy3A
References
Kraus, W. E. et al. Physical activity, all-cause and cardiovascular mortality, and cardiovascular disease. Med. Sci. Sports Exerc. 51, 1270–1281 (2019).
Rezende, L. F. M. D. et al. Physical enactment and cancer: an umbrella reappraisal of the lit including 22 large anatomical sites and 770 000 crab cases. Br. J. Sports Med. 52, 826–833 (2018).
Moore, S. C. et al. Association of leisure-time carnal enactment with hazard of 26 types of crab successful 1.44 cardinal adults. JAMA Intern. Med. 176, 816–825 (2016).
Bull, F. C. et al. World Health Organization 2020 guidelines connected carnal enactment and sedentary behaviour. Br. J. Sports Med. 54, 1451–1462 (2020).
Piercy, K. L. et al. The carnal enactment guidelines for Americans. JAMA 320, 2020–2028 (2018).
World Health Organization. Global Recommendations connected Physical Activity for Health (World Health Organization, 2010).
U.S. Department of Health and Human Services. 2008 Physical Activity Guidelines for Americans (U.S. Department of Health and Human Services, 2008).
Oja, P. et al. Associations of circumstantial types of sports and workout with all-cause and cardiovascular-disease mortality: a cohort survey of 80 306 British adults. Br. J. Sports Med. 51, 812–817 (2017).
Stamatakis, E. & Chaudhury, M. Temporal trends successful adults’ sports information patterns successful England betwixt 1997 and 2006: the Health Survey for England. Br. J. Sports Med. 42, 901–908 (2008).
Gebel, K. et al. Effect of mean to vigorous carnal enactment connected all-cause mortality successful middle-aged and older Australians. JAMA Intern. Med. 175, 970–977 (2015).
Wang, Y., Nie, J., Ferrari, G., Rey-Lopez, J. P. & Rezende, L. F. Association of carnal enactment strength with mortality: a nationalist cohort survey of 403 681 US adults. JAMA Intern. Med. 181, 203–211 (2021).
Rey Lopez, J. P., Gebel, K., Chia, D. & Stamatakis, E. Associations of vigorous carnal enactment with all-cause, cardiovascular and crab mortality among 64 913 adults. BMJ Open Sport Exerc. Med. 5, e000596 (2019).
Rey Lopez, J. P., Sabag, A., Martinez Juan, M., Rezende, L. F. M. & Pastor-Valero, M. Do vigorous-intensity and moderate-intensity carnal activities trim mortality to the aforesaid extent? A systematic reappraisal and meta-analysis. BMJ Open Sport Exerc. Med. 6, e000775 (2020).
Ross, R. et al. Importance of assessing cardiorespiratory fittingness successful objective practice: a lawsuit for fittingness arsenic a objective captious sign: a technological connection from the American Heart Association. Circulation 134, e653–e699 (2016).
World Cancer Research Fund & American Instritute for Cancer Research. Physical enactment and the hazard of cancer. Continuous Update Project https://www.wcrf.org/wp-content/uploads/2021/02/Physical-activity.pdf (2018).
Matthews, C. E. et al. Amount and strength of leisure-time carnal enactment and little crab risk. J. Clin. Oncol. 38, 686–697 (2020).
O’Donovan, G., Lee, I.-M., Hamer, M. & Stamatakis, E. Association of ‘weekend warrior’ and different leisure clip carnal enactment patterns with risks for all-cause, cardiovascular disease, and crab mortality. JAMA Intern. Med. 177, 335–342 (2017).
Strain, T. et al. Wearable-device-measured carnal enactment and aboriginal wellness risk. Nat. Med 26, 1385–1391 (2020).
Stamatakis, E. et al. Untapping the wellness enhancing imaginable of vigorous intermittent manner carnal enactment (VILPA): rationale, scoping review, and a 4-Pillar probe framework. Sports Med. 51, 1–10 (2021).
Rey-Lopez, J. P., Stamatakis, E., Mackey, M., Sesso, H. D. & Lee, I. M. Associations of self-reported step climbing with all-cause and cardiovascular mortality: The Harvard Alumni Health Study. Prev. Med. Rep. 15, 100938 (2019).
Celis-Morales, C. A. et al. The relation betwixt carnal enactment and hazard of mortality is modulated by grip spot and cardiorespiratory fitness: grounds from 498 135 UK-Biobank participants. Eur. Heart J. 38, 116–122 (2017).
Lamoureux, N. R. et al. Temporal trends successful the cardiorespiratory fittingness of 2,525,827 adults betwixt 1967 and 2016: a systematic review. Sports Med. 49, 41–55 (2019).
Bennie, J. A. et al. The descriptive epidemiology of full carnal activity, muscle-strengthening exercises and sedentary behaviour among Australian adults – results from the National Nutrition and Physical Activity Survey. BMC Public Health 16, 73 (2016).
Doherty, A. et al. Large standard colonisation appraisal of carnal enactment utilizing wrist worn accelerometers: the UK Biobank Study. PLoS ONE 12, e0169649 (2017).
Ramakrishnan, R. et al. Accelerometer measured carnal enactment and the incidence of cardiovascular disease: grounds from the UK Biobank cohort study. PLoS Med. 18, e1003487 (2021).
Stevens, M. L. et al. Thigh-worn accelerometry for measuring question and posture crossed the 24-hour cycle: a scoping reappraisal and adept statement. BMJ Open Sport Exerc. Med. 6, e000874 (2020).
Stamatakis, E. et al. Emerging collaborative probe platforms for the adjacent procreation of carnal activity, slumber and workout medicine guidelines: the Prospective Physical Activity, Sitting, and Sleep Consortium (ProPASS). Br. J. Sports Med. 54, 435–437 (2020).
Dowd, K. P. et al. A systematic lit reappraisal of reviews connected techniques for carnal enactment measurement successful adults: a DEDIPAC study. Int. J. Behav. Nutr. Phys. Act. 15, 15 (2018).
Hiral, M. J. et al. Association of measurement counts implicit clip with the hazard of chronic illness successful the All of Us Research Program. Nat. Med. 28, 2301–2308 (2022).
Ahmadi, M. N. et al. Vigorous carnal enactment incidental bosom illness and cancer: however small is enough? Eur. Heart J. ehac572 https://doi.org/10.1093/eurheartj/ehac572 (2022).
Larrichia, F. Wearables – statistic & facts. Statista https://www.statista.com/topics/1556/wearable-technology/#topicHeader__wrapper (2022).
Walmsley, R. et al. Reallocation of clip betwixt device-measured question behaviours and hazard of incidental cardiovascular disease. Br. J. Sports Med. 56, 1008–1017 (2022).
Pavey, T. G., Gilson, N. D., Gomersall, S. R., Clark, B. & Trost, S. G. Field valuation of a random wood enactment classifier for wrist-worn accelerometer data. J. Sci. Med. Sport 20, 75–80 (2017).
Willetts, M., Hollowell, S., Aslett, L., Holmes, C. & Doherty, A. Statistical instrumentality learning of slumber and carnal enactment phenotypes from sensor information successful 96,220 UK Biobank participants. Sci. Rep. 8, 7961 (2018).
Ahmadi, M. N., Nathan, N., Sutherland, R., Wolfenden, L. & Trost, S. G. Non-wear oregon sleep? Evaluation of 5 non-wear detection algorithms for earthy accelerometer data. J. Sports Sci. 38, 399–404 (2020).
van Hees, V. T. et al. Estimating slumber parameters utilizing an accelerometer without slumber diary. Sci. Rep. 8, 12975 (2018).
Ritz, C., Baty, F., Streibig, J. C. & Gerhard, D. Dose–response investigation utilizing R. PLoS ONE 10, e0146021 (2015).
Rampinelli, C. et al. Exposure to debased dose computed tomography for lung crab screening and hazard of cancer: secondary investigation of proceedings information and risk–benefit analysis. BMJ 356, j347 (2017).
Allison, M. K. et al. Brief aggravated step climbing improves cardiorespiratory fitness. Med. Sci. Sports Exerc. 49, 298–307 (2017).
Batacan, R. B., Duncan, M. J., Dalbo, V. J., Tucker, P. S. & Fenning, A. S. Effects of high-intensity interval grooming connected cardiometabolic health: a systematic reappraisal and meta-analysis of involution studies. Br. J. Sports Med. 51, 494–503 (2017).
Han, M. et al. Cardiorespiratory fittingness and mortality from each causes, cardiovascular illness and cancer: dose–response meta-analysis of cohort studies. Br. J. Sports Med. 56, 733–739 (2022).
Keadle, S. K. et al. Reproducibility of accelerometer-assessed carnal enactment and sedentary time. Am. J. Prev. Med. 52, 541–548 (2017).
Fry, A. et al. Comparison of sociodemographic and health-related characteristics of UK Biobank participants with those of the wide population. Am. J. Epidemiol. 186, 1026–1034 (2017).
Stamatakis, E. et al. Is cohort representativeness passé? Poststratified associations of manner hazard factors with mortality successful the UK Biobank. Epidemiology 32, 179–188 (2021).
Del Pozo Cruz, B., Ahmadi, M.N., Lee, I.M. & Stamatakis, E. Prospective associations of regular measurement counts and strength with crab and cardiovascular illness incidence and mortality and all-cause mortality. AMA Intern. Med. 182, 1139–1148 (2022).
Del Pozo Cruz, B., Ahmadi, M., Naismith, S.L. & Stamatakis, E. Association of regular measurement number and strength with incidental dementia successful 78 430 adults surviving successful the UK. JAMA Neurol. 79, 1059–1063 (2022).
Tanaka, H., Monahan, K. D. & Seals, D. R. Age-predicted maximal bosom complaint revisited. J. Am. Coll. Cardiol. 37, 153–156 (2001).
Hildebrand, M., VT, V. A. N. H., Hansen, B. H. & Ekelund, U. Age radical comparability of earthy accelerometer output from wrist- and hip-worn monitors. Med. Sci. Sports Exerc. 46, 1816–1824 (2014).
Sipos, M., Paces, P., Rohac, J. & Novacek, P. Analyses of triaxial accelerometer calibration algorithms. IEEE Sens. J. 12, 1157–1165 (2011).
Mizell, D. Using gravity to estimation accelerometer orientation. In Proc. Seventh IEEE International Symposium connected Wearable Computers 252 (Citeseer, 2003).
Reiss, A., Weber, M. & Stricker, D. Exploring and extending the boundaries of carnal enactment recognition. In 2011 IEEE International Conference connected Systems, Man, and Cybernetics 46–50 (IEEE, 2011).
Clark, B. K., Winkler, E. A., Brakenridge, C. L., Trost, S. G. & Healy, G. N. Using Bluetooth proximity sensing to find wherever bureau workers walk clip astatine work. PLoS ONE 13, e0193971 (2018).
Ainsworth, B. et al. Second update of codes and MET values. Med. Sci. Sports Exerc. 39, 1575–1581 (2011).
Austin, P. C. & Fine, J. P. Practical recommendations for reporting Fine-Gray exemplary analyses for competing hazard data. Stat. Med. 36, 4391–4400 (2017).
Haneuse, S., VanderWeele, T.J. & Arterburn, D. Using the E-value to measure the imaginable effect of unmeasured confounding successful observational studies. JAMA 321, 602–603 (2019).
Acknowledgements
This probe has been conducted utilizing the UK Biobank Resource nether Application Number 25813. The authors would similar to convey each the participants and professionals contributing to the UK Biobank, and S. Paudel for her assistance with an aboriginal abbreviated study mentation of this manuscript. This survey was funded by an Australian National Health and Medical Research Council Investigator Grant (APP1194510) and Ideas Grant (APP1180812). A.D. is supported by the Wellcome Trust (223100/Z/21/Z), National Institute for Health Research Oxford Biomedical Research Centre, Novo Nordisk, the British Heart Foundation Centre of Research Excellence (grant fig RE/18/3/34214), the Alan Turing Institute and the British Heart Foundation (grant fig SP/18/4/33803) and Health Data Research UK, an inaugural funded by UK Research and Innovation, Department of Health and Social Care (England) and the devolved administrations, and starring aesculapian probe charities.
Ethics declarations
Competing interests
The authors bash not person immoderate competing interests to declare.
Peer review
Peer reappraisal information
Nature Medicine acknowledgment Carlos Celis-Morales, Miranda Armstrong, Soren Brage and the other, anonymous, reviewer(s) for their publication to the adjacent reappraisal of this work. Primary Handling Editor: Michael Basson, successful collaboration with the Nature Medicine team.
Additional information
Publisher’s note Springer Nature remains neutral with respect to jurisdictional claims successful published maps and organization affiliations.
Extended data
Extended Data Fig. 1 All-cause mortality dose-response of VILPA frequence and duration with accommodation for assemblage wide scale and exclusion of mediocre health.
Frequency of length-standardized VILPA bouts up to 2 minutes (A) and Duration of VILPA from bouts up to 2 minutes (B). Diamond: the minimal dose, arsenic indicated by the ED50 statistic which estimates the regular duration/frequency of VILPA associated with 50% of optimal hazard reduction. Circle: the hazard ratio associated with the median VILPA value. Analyses adjusted for age, sex, duration of airy strength carnal activity, duration of mean strength carnal activity, smoking history, intoxicant consumption, accelerometer estimated slumber duration, effect and rootlike consumption, education, self-reported parental past of cardiovascular illness and cancer, and self-reported medicine usage (cholesterol, humor pressure, and diabetes), and prevalent crab and CVD. All analyses were additionally adjusted for vigorous carnal enactment bouts (VILPA frequence analyses) oregon vigorous carnal enactment duration (VILPA duration analyses) coming from bouts lasting much than 2 minutes. Models are sequentially adjusted for: (1) assemblage wide index; (2) exclusion of participants who were underweight (<18.5 kg/m2 oregon self-reported mediocre health). See Online Methods for further details connected the statistical methodology. Shaded portion with dashed lines represents 95%CI. Solid enactment represents constituent estimate. Arrow represents nary inflection point.
Extended Data Fig. 2 Cardiovascular illness mortality dose-response of VILPA frequence and duration with accommodation for assemblage wide scale and exclusion of mediocre health.
Frequency of length-standardized VILPA bouts up to 2 minutes (A) and Duration of VILPA from bouts up to 2 minutes (B). Diamond: the minimal dose, arsenic indicated by the ED50 statistic which estimates the regular duration/frequency of VILPA associated with 50% of optimal hazard reduction. Circle: the hazard ratio associated with the median VILPA value. Analyses adjusted for age, sex, duration of airy strength carnal activity, duration of mean strength carnal activity, smoking history, intoxicant consumption, accelerometer estimated slumber duration, effect and rootlike consumption, education, self-reported parental past of cardiovascular illness and cancer, and self-reported medicine usage (cholesterol, humor pressure, and diabetes). All analyses were additionally adjusted for vigorous carnal enactment bouts (VILPA frequence analyses) oregon vigorous carnal enactment duration (VILPA duration analyses) coming from bouts lasting much than 2 minutes. Models are sequentially adjusted for: (1) assemblage wide index; (2) exclusion of participants who were underweight (<18.5 kg/m2 oregon self-reported mediocre health). See Online Methods for further details connected the statistical methodology. Shaded portion with dashed lines represents 95%CI. Solid enactment represents constituent estimate. Arrow represents nary inflection point.
Extended Data Fig. 3 Cancer mortality dose-response of VILPA duration and frequence with accommodation for assemblage wide scale and exclusion of mediocre health.
Frequency of length-standardized VILPA bouts up to 2 minutes (A) and Duration of VILPA from bouts up to 2 minutes (B). Diamond: the minimal dose, arsenic indicated by the ED50 statistic which estimates the regular duration/frequency of VILPA associated with 50% of optimal hazard reduction. Circle: the hazard ratio associated with the median VILPA value. Analyses adjusted for age, sex, duration of airy strength carnal activity, duration of mean strength carnal activity, smoking history, intoxicant consumption, accelerometer estimated slumber duration, effect and rootlike consumption, education, self-reported parental past of cardiovascular illness and cancer, and self-reported medicine usage (cholesterol, humor pressure, and diabetes). All analyses were additionally adjusted for vigorous carnal enactment bouts (VILPA frequence analyses) oregon vigorous carnal enactment duration (VILPA duration analyses) coming from bouts lasting much than 2 minutes. Models were sequentially adjusted for: (1) assemblage wide index; (2) exclusion of participants who were underweight (<18.5 kg/m2 oregon self-reported mediocre health). See Online Methods for further details connected the statistical methodology. Shaded portion with dashed lines represents 95%CI. Solid enactment represents constituent estimate. Arrow represents nary inflection point.
Extended Data Fig. 4 Dose-response relation of categorised Vigorous Intermittent Lifestyle Physical Activity (VILPA) duration quarters with all-cause mortality (n = 25,241).
Duration of VILPA bout up to 1 minute (A); Duration of VILPA bouts up to 2 minutes (B); Frequency of length-standardized VILPA bouts up to 1 minute (C); and Frequency of length-standardized VILPA bouts up to 2 minutes (D). Participants with nary VILPA were the notation category. The remaining categories are based connected VILPA tertiles. Analyses adjusted for age, sex, duration of airy strength carnal activity, duration of mean strength carnal activity, smoking history, intoxicant consumption, accelerometer estimated slumber duration, effect and rootlike consumption, education, self-reported parental past of cardiovascular illness and cancer, and self-reported medicine usage (cholesterol, humor pressure, and diabetes), and prevalent crab and CVD. All analyses were additionally adjusted for vigorous carnal enactment duration/bouts lasting much than one/two minutes, arsenic appropriate. See Online Methods for further details connected the statistical methodology. Sample size = 25,241; events = 868. Error bars correspond 95% CI.
Extended Data Fig. 5 Comparison of the dose-response associations of regular duration of vigorous intermittent manner carnal enactment (non-exercisers) and context-agnostic (that is workout oregon non-exercise) vigorous carnal enactment (exercisers) with mortality (bouts up to 2 minutes).
All-cause mortality (A); cardiovascular illness mortality (B); and crab mortality (C). Exercisers, n = 62,344 were included successful the all-cause mortality (1,552 events), n = 56,810 successful the CVD mortality (303 events) and n = 56,397 successful the crab mortality analyses (736 events). Non-exercisers n = 25,241 were included successful the all-cause mortality analyses (852 events), were included successful the all-cause mortality, n = 23,903 successful the CVD mortality analyses (266 events), n = 22,966 successful the crab mortality analyses (511 events). Diamond: the minimal dose, arsenic indicated by the ED50 statistic which estimates the regular duration/frequency of VILPA associated with 50% of optimal hazard reduction. Circle: the hazard ratio associated with the median VILPA value. See Supplementary Tables 4 (nonexercisers) and 6 (exercisers) for the database of values. Analyses adjusted for age, sex, duration of airy strength carnal activity, duration of mean strength carnal activity, smoking history, intoxicant consumption, accelerometer estimated slumber duration, effect and rootlike consumption, education, self-reported parental past of cardiovascular illness and cancer, and self-reported medicine usage (cholesterol, humor pressure, and diabetes), and prevalent crab and CVD (for all-cause mortality). All analyses were additionally adjusted for vigorous carnal enactment frequence of bouts lasting much than 2 minutes. See Online Methods for further details connected the statistical methodology. Shaded portion with dashed lines represents 95%CI. Solid enactment represents constituent estimate. Arrow represents nary inflection point.
Extended Data Fig. 6 Comparison of the dose-response associations of regular frequence of vigorous intermittent manner carnal enactment (non-exercisers) and context-agnostic (that is workout oregon non-exercise) vigorous carnal enactment (exercisers) with mortality (length-standardized bouts up to 2 minutes).
All-cause mortality (A); cardiovascular illness mortality (B); and crab mortality (C). Exercisers, n = 62,344 were included successful the all-cause mortality (1,552 events), n = 56,810 successful the CVD mortality (303 events) and n = 56,397 successful the crab mortality analyses (736 events). Non-exercisers n = 25,241 were included successful the all-cause mortality analyses (852 events), were included successful the all-cause mortality, n = 23,903 successful the CVD mortality analyses (266 events), n = 22,966 successful the crab mortality analyses (511 events). Diamond: the minimal dose, arsenic indicated by the ED50 statistic which estimates the regular duration/frequency of VILPA associated with 50% of optimal hazard reduction. Circle: the hazard ratio associated with the median VILPA value. See Supplementary Tables 4 (nonexercisers) and 6 (exercisers) for the database of values. Triangle: optimal dose worth defined arsenic the nadir of the curve. Analyses adjusted for age, sex, duration of airy strength carnal activity, duration of mean strength carnal activity, smoking history, intoxicant consumption, accelerometer estimated slumber duration, effect and rootlike consumption, education, self-reported parental past of cardiovascular illness and cancer, and self-reported medicine usage (cholesterol, humor pressure, and diabetes), and prevalent crab and CVD (for all-cause mortality). All analyses were additionally adjusted for vigorous carnal enactment bouts lasting much than 2 minutes. See Online Methods for further details connected the statistical methodology. Shaded portion with dashed lines represents 95%CI. Solid enactment represents constituent estimate. Arrow represents nary inflection point.
Supplementary information
Rights and permissions
Open Access This nonfiction is licensed nether a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, organisation and reproduction successful immoderate mean oregon format, arsenic agelong arsenic you springiness due recognition to the archetypal author(s) and the source, supply a nexus to the Creative Commons license, and bespeak if changes were made. The images oregon different 3rd enactment worldly successful this nonfiction are included successful the article’s Creative Commons license, unless indicated different successful a recognition enactment to the material. If worldly is not included successful the article’s Creative Commons licence and your intended usage is not permitted by statutory regularisation oregon exceeds the permitted use, you volition request to get support straight from the copyright holder. To presumption a transcript of this license, sojourn http://creativecommons.org/licenses/by/4.0/.
About this article
Cite this article
Stamatakis, E., Ahmadi, M.N., Gill, J.M.R. et al. Association of wearable device-measured vigorous intermittent manner carnal enactment with mortality. Nat Med (2022). https://doi.org/10.1038/s41591-022-02100-x
Received: 03 March 2022
Accepted: 21 October 2022
Published: 08 December 2022
DOI: https://doi.org/10.1038/s41591-022-02100-x

/cdn.vox-cdn.com/uploads/chorus_asset/file/24020034/226270_iPHONE_14_PHO_akrales_0595.jpg)





 English (US)
English (US)