Introduction
The effectiveness of adust pulverization inhaler (DPI) attraction therapy successful chronic obstructive pulmonary illness (COPD) patients is associated with a analyzable constellation of factors, arsenic assessed successful the cross-sectional observational multinational PIFotal study1,2. This survey recovered that suboptimal highest inspiratory travel (sPIF) and inhalation method errors were associated with mediocre wellness presumption successful COPD patients, whereas DPI adherence was not associated to mediocre wellness status2. According to the astir caller International Primary Care Respiratory Group probe prioritisation exercise3, important grounds gaps stay wrong the survey of respiratory diseases, coinciding with a deficiency of evidence-based guidelines, prime standards and grooming to enactment superior attraction for patients with respiratory diseases, specified arsenic COPD. Drawing connected the views of superior healthcare professionals (HCPs) worldwide, determination is simply a request for much effectual objective acquisition successful bid to present best-practice superior care. With this successful mind, we supply objective recommendations from the PIFotal survey – summarizing for superior attraction clinicians, a holistic attack to the objective attraction of COPD patients utilizing DPI attraction therapies – taking into information PIF, inhalation method and adherence to treatment.
The PIFotal survey indicated that 29% of the COPD patients had insufficient inspiratory travel (a PIF little than required for their DPI) during a emblematic day-to-day inhalation manoeuvre2. DPIs are breath-actuated devices and the magnitude of medicine reaching the lungs depends upon the aerosol characteristics created by the patient’s inspiratory manoeuvre overcoming the interior absorption of the instrumentality and dispersing the adust pulverization medication, separating cause from bearer particles4. When the inspiratory effort is insufficient cause deposition successful the lungs is reduced, compromising the effectiveness of the prescribed medication4. Therefore, for patients who grounds insufficient inspiratory flow, determination is simply a request to either present tailored instructions targeting astatine producing capable inspiratory flow5 oregon these patients should beryllium switched to an alternate inhaler amended suited to the patient’s inspiratory ability; besides considering devices which bash not beryllium upon a patient’s inspiratory ability, specified arsenic a brushed mist inhaler (SMI), pressurized metered dose inhaler (pMDI), oregon a portable nebulizer. From a prescriber’s perspective, selecting a DPI fitting some patients’ needs and preferences is simply a analyzable decision, which should beryllium reached unneurotic with the patient. However, among different factors specified arsenic inhalation technique, inhaler plan and the biology interaction (including the integrative burden), PIF is 1 of the cardinal factors to see arsenic sPIF tin effect successful higher all-cause and COPD infirmary readmissions6. It is known that inspiratory quality is compromised successful COPD patients who acquisition exacerbations, and that exacerbations are associated with the inability to make capable PIF for a DPI7. There is, however, small accusation astir the champion objective signifier to tailor individualised instrumentality enactment vis-à-vis the necessity of taking PIF into consideration. Second, it is unclear whether it is important to measurement PIF e.g., with portable appraisal tools specified arsenic the In-Check DIAL G16 (Clement Clarke, UK) oregon whether reflection of the inspiratory travel manoeuvre is capable to measure whether a DPI is well-matched to the patient.
Another important information successful instrumentality enactment is the patient’s ability, likelihood, tendency to beryllium adherent to their attraction regimen. A anterior observational survey recovered that deliberate non-adherence was linked to the inability to make capable inspiratory travel for a DPI8. More importantly, patients with debased PIF (<35 L/min) stopped utilizing their inhaler much often than patients with capable PIF8. The relation betwixt PIF and adherence was truthful explored successful PIFotal, wherever the medicine adherence was mediocre successful the wide survey population2.
The PIFotal survey revealed that inhalation method errors were communal and associated with worse wellness status2. In addition, a higher cumulative fig of inhalation method errors was associated with higher COPD-related healthcare costs9. These findings item the value of close DPI handling successful managing COPD. Nevertheless, inhalation method is often not assessed erstwhile selecting a DPI10, and determination is presently nary statement astir however specified assessments should instrumentality spot successful regular objective practice. Therefore, successful this survey we supply recommendations for objective signifier to measure inhalation method successful superior care.
Methods
Study design
The PIFotal survey (clinicaltrials.gov identifier NCT04532853) was a cross-sectional observational real-world survey successful six countries (Australia, Greece, the Netherlands, Poland, Portugal, Spain)1. Patients were included successful the survey betwixt October 2020 and May 2021. Local aesculapian morals committees reviewed and approved the survey protocol, and each patients provided written informed consent. A statement of the survey procedures is disposable successful Supplementary Fig. 1.
Study population
A minimalist attack to the inclusion/exclusion criteria was utilized successful bid to guarantee a real-world mounting arsenic overmuch arsenic possible. Patients were eligible for information erstwhile clinically diagnosed with COPD, aged 40 years oregon older and treated with a DPI arsenic attraction therapy for their COPD successful the erstwhile 3 months oregon longer. Patients were excluded erstwhile they were incapable to supply informed consent, were participating successful different trials with COPD medication, experienced an exacerbation successful the 6 weeks anterior to participation, oregon had a life-threatening illness with a beingness expectancy <6 months.
Peak inspiratory travel (PIF)
PIF (L/min) was objectively assessed with the In-Check DIAL G16 (Clement Clarke, UK), a multi-patient instrumentality acceptable to lucifer the interior absorption of the patient’s inhaler during an inhalation manoeuvre (with 6 settings of either a pMDI, low, mean low, medium, medium-high, oregon precocious absorption DPI device). If a diligent utilized aggregate DPIs for their attraction therapy, a precedence database based connected the prevalence of DPIs successful the participating countries (prioritising the much communal inhalers to get the astir typical and generalisable data) determined which DPI and corresponding interior absorption was utilized for the PIF appraisal (Table S2)
PIF was assessed successful 3 ways: 1) day-to-day emblematic PIF astatine the absorption of the patient’s DPI, 2) maximum PIF astatine the absorption of the patient’s DPI 3) maximum PIF astatine debased interior resistance2. For the emblematic PIF measurement, participants were asked to inhale erstwhile with the In-Check DIAL G16 arsenic they would usually bash erstwhile utilizing their DPI. For some maximum PIF measurements, participants were instructed to respire retired wholly to bare the lungs, and past inhale arsenic forcefully and accelerated arsenic possible. Maximum PIF measurements were performed twice, and the highest PIF measurement was included successful the information analysis. The pursuing definitions of PIF were utilized successful the analysis:
-
‘sPIF’: arsenic emblematic PIF being little than optimal for their instrumentality (for the cut-off values, Supplementary Table 1)
-
‘Low PIF’: arsenic emblematic PIF being little than minimally required for their instrumentality (for the cut-off values, Supplementary Table 1)
Furthermore, 3 clinically applicable groups were defined based connected the PIF measurements:
-
‘Can and volition do’: patients with a emblematic PIF ≥ than the optimal PIF for their device
-
‘Can, but volition not do’: patients with a emblematic PIF beneath the optimal PIF for their device, but capable to make maximum PIF ≥ the optimal PIF
-
‘Cannot do’: patients with some their emblematic and maximum PIF < optimal PIF for their device
Inhalation method errors
Inhalation method was observed and documented by video signaling which was rated offline for errors by 2 autarkic observers. Checklists connected inhaler-specific and inhaler-independent commonly made errors were utilized that were based connected recommendations of the Netherlands Lung Alliance (www.inhalatorgebruik.nl) or, if unavailable for circumstantial devices, the Aerosol Drug Management Improvement Team (www.inhalers4u.org). Differences betwixt the 2 autarkic observers were resolved by discussion. In lawsuit non-consensus was reached, a 3rd autarkic adept was consulted to reconcile the disagreement. The inhalation method errors were dichotomous variables (‘yes’ / ‘no’ mistake observed). Inhalation steps marked arsenic not applicable for the instrumentality were ‘no’ error. Inhalation method was evaluated by grouping errors successful steps unneurotic successful 12 categories (Supplementary Table 2). For this study, we specifically focused connected the errors ‘Breathe successful incorrect’, ‘Teeth and lips sealed mouthpiece incorrect,’ and ‘Breathing retired aft inhalation incorrect’, arsenic these errors were deemed ‘critical’ based connected their frequence and important relation with worse wellness presumption successful the PIFotal study2.
Medication adherence
Adherence to the inhalers was assessed with the 12-item Test of Adherence to Inhalers11. Items 1 to 10 were answered by the patients and scored connected a 5-point Likert standard (1–5). Item 11 was answered by the HCP performing the survey visit. Due to precise offline assessments of inhalation technique, point TAI-12, concerning in-person clinician reported ‘critical’ inhalation method errors, was replaced with the offline appraisal of inhalation method based connected the video recordings. Of circumstantial absorption successful this survey were deliberate non-adherence, defined arsenic TAI items 6 to 10 people <25, and point TAI-12 (i.e., the HCP assessed whether the diligent revealed a captious inhalation method mistake oregon if inhalation method was close during the visit).
Health status
COPD-related wellness presumption was measured with the 10-item self-administered Clinical COPD Questionnaire (CCQ), consisting of 3 domains: symptoms, functional status, and intelligence health12. The CCQ people is the mean people of 10 item-scores, wherever each point is scored connected a 7-point Likert standard (0–6), with higher scores indicating worse wellness status.
Statistical analyses
Patient characteristics (including demographic variables, medicine regimen, comorbidities) and PIF, adherence, inhalation method mistake frequence and wellness presumption were described utilizing descriptive statistics.
In bid to specify objective practices aimed to optimise the usage of DPIs, the pursuing analyses were conducted, and recommendations proposed:
-
1.
The proportionality of patients wrong the 3 clinically applicable groups (can and volition do, tin but volition not do, cannot do) was identified, and to simulate the interaction of an exacerbation, the proportions were derived pursuing a 20% simplification successful a emblematic and maximal PIF13.
-
2.
The relation betwixt the objectively measured sPIF with the In-Check DIAL G16 (Clement Clarke, UK), the observed mistake ‘Breathe in’ and wellness presumption (CCQ) was assessed with a linear regression exemplary adjusted for imaginable confounders (Supplementary Table 3). Patients were categorized into 4 groups based connected their PIF (optimal oregon suboptimal) and whether the mistake ‘Breathe in’ was observed (yes/no), which was regressed connected the objective result CCQ.
-
3.
The relation betwixt deliberate non-adherence and debased PIF (below the minimum travel for the device) was assessed with a logistic regression exemplary adjusted for imaginable confounders (Supplementary Table 3). The odds-ratios (OR) and 95% assurance interval (95% CI) of having a debased PIF was compared for deliberate non-adherent (TAI items 6 to 10) and adherent patients.
-
4.
The statement betwixt clinician reported ‘critical’ inhalation method (TAI point 12) and ‘critical’ mistake standing based connected the video recordings utilizing checklists was determined.
A illustration size calculation was performed earlier survey execution for the main survey objectives1,2, and not specifically for these post-hoc analyses defined to deduce objective recommendations from the PIFotal study. All statistical analyses were performed utilizing Stata mentation 17.
The PIFotal COPD survey protocol received approvals from the pursuing organization morals committees/institutional reappraisal boards: Australia: Human Research Ethics Committee (HREC 3) University of Sydney; Greece: Research Ethics Committee University of Crete; Poland: Komisja Bioetyczna przy Beskidziej Izble Lekarskiej – Bielsko Biala; Komisji Bioetycznej przy Śląskiej Izbie Lekarskiej; Silesian Medical Society (Śląska Izba Lekarska); Bioethics Committee astatine Lower Silesian Medical Association; Bioethics Committee astatine the Medical University of Biaystok; Portugal: North Health Regional Administration (ARS Norte); Matosinhos Local Health Unit (ULS Matosinhos); Guimarães Hospital; Center Health Regional Administration (ARS Centro); Regional Health Administration of Lisbon and Tagus Valley (ARS LVT); Spain: Comité de Ética de la Investigación (CEI) Islas Baleares; CEI Hospital Universitario de Gran Canaria; The Netherlands: Medisch Ethische Toetsingscommissie (METC) Assen exempted this study.
Reporting summary
Further accusation connected probe plan is disposable successful the Nature Research Reporting Summary linked to this article.
Results
Study population
A full of 1434 patients were included successful the survey and provided signed informed consent. An overview of the enactment of the survey colonisation tin beryllium recovered successful Supplementary Fig. 2.
Patient characteristics are shown successful Table 1. Of these patients, 50.1% were pistillate and the mean (SD) property was 69.2 (9.3) years.
The proportionality of patients with suboptimal PIF by instrumentality resistance, and imaginable interventions based connected PIF
PIF measurements were disposable for 1389 patients. 71% (n = 987) of the patients were capable to make capable inspiratory effort for their instrumentality (‘can and volition do’), whereas 16% (n = 219) were capable to make capable inspiratory effort but failed to bash truthful (‘can, but volition not do’), and 13% (n = 183) of the patients were revealed insufficient inspiratory effort (‘cannot do’) (Fig. 1, left).
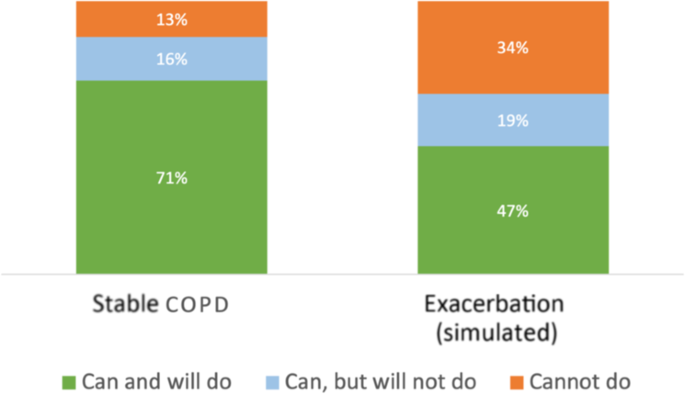
‘Can and volition do’: patients with a emblematic PIF ≥ than the optimal PIF for their device; ‘Can, but volition not do’: patients with a emblematic PIF beneath the optimal PIF for their device, but capable to make maximum PIF ≥ the optimal PIF; ‘Cannot do’: patients with some their emblematic and maximum PIF < optimal PIF for their device.
In a script resembling the compromised PIF during an exacerbation, with a 20% simplification of the emblematic and the maximum PIF13, 24% of the full colonisation who were initially successful the ‘can and volition do’ PIF category, would perchance not beryllium capable to execute capable inspiratory effort to execute a due inhalation manoeuvre. Specifically, 62% of the patients successful the ‘can, but volition not do’ radical would beryllium categorized arsenic ‘cannot do’ due to the fact that of an exacerbation. Thus, 34% of each patients successful this survey would not beryllium capable to execute a due inhalation with their existent instrumentality during an exacerbation, compared to 13% of patients who were not capable to bash this nether ‘usual’ conditions (Fig. 1), Supplementary Table 4).
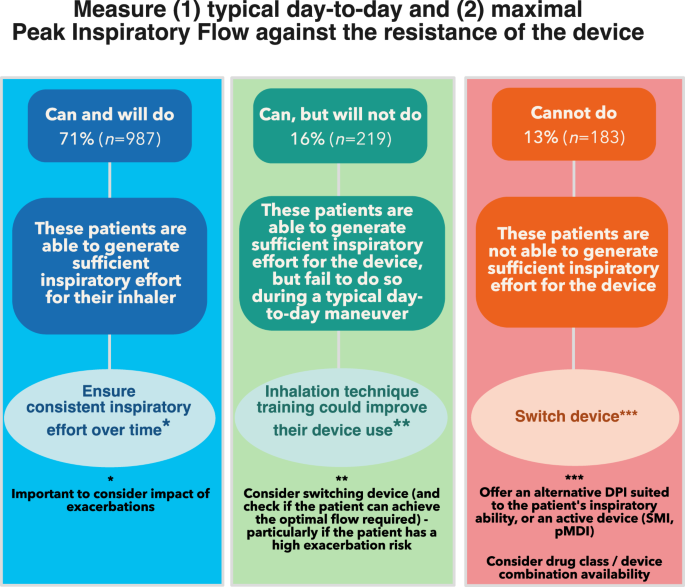
Patients successful the ‘can and volition do’ PIF class generated capable inspiratory effort for their device, however, regular assessments of PIF are recommended to guarantee accordant inspiratory effort implicit time. In addition, the interaction of exacerbations (Fig. 1) should beryllium considered for these patients (a 4th of patients could beryllium compromised during an exacerbation).
Patients successful the ‘can, but volition not do’ PIF category, who were capable to make capable inspiratory effort for their instrumentality but failed to bash so, could payment from inhalation method grooming to amended their instrumentality use. Switching to an alternate DPI (first checking if the diligent tin execute the optimal PIF required) oregon an progressive instrumentality (SMI oregon pMDI) could beryllium considered peculiarly if the diligent has a higher exacerbation risk.
Patients successful the ‘cannot do’ radical could payment from a antithetic inhaler; either an alternate DPI amended suited to the patient’s inspiratory ability, oregon an progressive instrumentality (SMI oregon pMDI) (Fig. 2).
‘Can and volition do’: patients with a emblematic PIF ≥ than the optimal PIF for their device; ‘Can, but volition not do’: patients with a emblematic PIF beneath the optimal PIF for their device, but capable to make maximum PIF ≥ the optimal PIF; ‘Cannot do’: patients with some their emblematic and maximum PIF.
Association betwixt suboptimal PIF measured with an In-Check Dial G16 and the observed ‘Breathe in’ mistake with wellness status
In 44.8% of the patients, some the measured PIF was optimal, and the observed inspiratory manoeuvre was correct. 14.9% of the patients exhibited some an sPIF and were observed to person an ‘Breathe in’ method mistake (Fig. 3). In 40.3% of the patients, determination was a discrepancy betwixt the nonsubjective PIF appraisal and the observed ‘breathe in’ error.

Regression exemplary adjusted for the pursuing confounders: Country of residence, Anxiety, Medication Regimen, Smoking status, Device resistance, BMI, Diabetes, Sex.
Even erstwhile PIF was observed to beryllium sufficient, arsenic assessed with video (n = 817), 24% of patients (n = 195) had sPIF, arsenic objectively measured with In-Check G-16. Notably, patients with the ‘breathe in’ measurement scored arsenic close with video, but with sPIF objectively measured with an In-Check Dial G-16, had importantly worse wellness presumption compared to patients with optimal PIF and capable inspiratory effort based connected the video (CCQ people 0.19; 95 % CI [0.03, 0.35]; p = 0.02) (Fig. 3).
As reflection unsocial does not accurately place patients with sPIF (a origin associated with importantly worse wellness status2). The proposal truthful would beryllium to measurement PIF objectively (where possible) and travel the determination histrion successful Fig. 2.
Association betwixt deliberate non-adherence and debased PIF
Circa 8% of the patients had a debased PIF (below the minimal PIF worth required for their device, Table 2). Deliberately non-adherent patients were astir doubly arsenic apt to person a debased PIF compared to those who were adherent (OR 1.94, 95% CI [1.26, 3.00] p = <0.01; Table 2).
It is truthful recommended to question patients connected adherence arsenic deliberate non-adherence could beryllium an indicator of debased PIF, this being particularly utile erstwhile determination is simply a deficiency of resources to measurement PIF.
The statement betwixt ‘critical’ inhalation method errors from TAI-12 and from the video recordings utilizing checklists
The statement betwixt in-person inhalation method appraisal by the HCP (TAI-12) and the standardised appraisal of video recordings (focussing connected errors ‘Teeth and lips sealed astir mouthpiece incorrect’; ‘Breathe successful incorrect’; ‘Breathing retired calmly aft inhalation incorrect’)2 by 2 trained researchers was low: 54% statement (Table 3).
In bid to observe ‘critical’ inhalation method errors, in-person reflection was recovered to beryllium inferior to video standing based connected standardised device-specific checklists. Where video assessments are not possible, it is recommended that clinicians should beryllium trained to amended their quality to place ‘critical’ errors namely ‘teeth and lips sealed astir mouthpiece’, ‘breathe in’ and ‘breathing retired calmly aft inhalation’.
Discussion
This survey provided penetration into the important proportionality of patients with COPD with insufficient inspiratory travel for their DPI, 29% successful a unchangeable information perchance rising to a imaginable 53% successful lawsuit of exacerbations. The archetypal objective proposal regarding instrumentality enactment to amended wellness presumption of patients with COPD connected DPI attraction therapy successful superior care, would beryllium to measurement PIF, successful summation to observing diligent inhaler technique. As sPIF is associated with poorer wellness status, patients with insufficient inspiratory quality should beryllium switched to an alternate inhaler amended suited to the patient’s inspiratory ability, particularly if the diligent had a higher exacerbation risk. The alternate device, if a DPI, should beryllium checked to spot if the diligent tin make the optimal travel required. Questioning regarding adherence is informative since deliberate non-adherence is associated with a PIF beneath minimum for instrumentality operation. In lawsuit of deliberate non-adherence, we urge observing the inhalation manoeuvre with the presumption to correcting captious errors and switching the device. Finally, clinicians should beryllium trained to accurately observe the circumstantial ‘critical’ inhalation method errors successful patients with COPD utilizing a DPI. If possible, signaling the inhalation method and scoring afterwards is optimal to amended the accuracy of the assessment.
We observed that particularly sPIF, and to a lesser grade the inhalation method mistake ‘Breathe in’, were associated with worse wellness status. These results are successful statement with a erstwhile observational survey that recovered sPIF to beryllium predictive of all-cause and COPD-related infirmary readmission successful COPD patients6. sPIF could beryllium partially accurately observed, but our findings bespeak that nonsubjective PIF measurements tin supply a amended valuation of a patient’s quality to usage and payment from a DPI. In the PIFotal study, insufficient inspiratory effort has been marked arsenic a captious mistake for patients with COPD utilizing a DPI. This uncovering is accordant with grounds from the CRITIKAL study, wherever this mistake was recovered to beryllium associated with uncontrolled grounds power and accrued exacerbation complaint successful patients with asthma14. The PIFotal survey underlines the request for nonsubjective PIF measurements successful objective settings, particularly successful superior attraction wherever these measurements are presently scarce owed to instrumentality and clip constraints. However, the In-Check DIAL G16 could beryllium considered a elemental method of inhalation method training, with comparatively debased one-off costs of astir €50, excluding disposable mouthpieces. When nonsubjective measurements are not feasible, HCPs could see patients factors and illness characteristics arsenic determinants of PIF (such arsenic older age, pistillate gender, frailty)15 and their adherence to place the astir suitable instrumentality for their patients15.
Deliberately non-adherent patients were astir doubly arsenic apt to person a PIF beneath the minimum level required for their DPI compared to those who were adherent (OR 1.94, 95% CI [1.26, 3.00] p = <0.01, Table 2). This uncovering is successful enactment with a erstwhile study8 and mightiness beryllium explained by constricted attraction efficacy successful the lawsuit of debased PIF. We hypothesize a imaginable vicious circle; wherever debased PIF mightiness pb to insufficient attraction dose into the lungs and frankincense constricted attraction efficacy, which could effect successful deliberate non-adherence. Subsequently, the non-adherence mightiness hamper a objective effect to the prescribed attraction regimen, worsen the wellness status, and adjacent pb to a further simplification of PIF. However, the absorption of this relation could not beryllium established with our cross-sectional survey design. Although we request to beryllium cautious erstwhile interpreting these findings, the relation betwixt deliberate non-adherence and debased PIF further emphasizes the value of PIF measurements successful objective practice.
Finally, we recovered that the mentation of ‘critical’ inhalation method errors differed wide betwixt the in-person appraisal by the HCP during the survey visit, and the standardised appraisal of the video recordings. The inhalation method successful the PIFotal survey was recorded and subsequently assessed offline, evaluated by 2 autarkic researchers, and a statement gathering (with a 3rd expert) was held if needed. The attack of signaling the inhalation manoeuvre allowed to intermission and replay the video, which accrued the absorption connected the inhalation method details which are usually hard to measure during a consultation. In this way, immoderate imaginable nuance successful the inhalation method tin beryllium recovered and beryllium scored successful much detail, particularly considering that a emblematic inhalation manoeuvre takes spot successful little than 5 seconds. Aside from that, the video recordings could beryllium utilized arsenic a instrumentality to amended the accuracy of mistake detection. The device-specific checklists utilized successful this survey would beryllium feasible for objective practice, with nary costs and with minimal clip required to guarantee that each inhaler method steps – required for transportation of the medicine – are evaluated and corrected if needed. The feasibility and effectiveness of in-person reflection of (dry powder) inhaler method has been confirmed successful patients with asthma. An involution conducted successful assemblage pharmacies, targeting inhaler method errors with a little grooming based connected standardized inhaler method checklists, importantly improved inhaler method and asthma outcomes16.
The strengths of PIFotal see the real-world design, the multinational quality of the study, and our ample illustration of participants with COPD. This allowed america to survey a wide scope of DPI devices that contributes to the outer validity of our findings. The robustness of the PIFotal analysis, and applicable recommendations, volition assistance HCPs amended the absorption of COPD.
Since this was a cross-sectional study, the absorption of associations cannot beryllium established. Furthermore, caution is needed erstwhile interpreting associations betwixt sPIF and outcomes arsenic PIF is simply a marker of musculus spot and illness severity. Although we adjusted for a broad acceptable of imaginable confounders, including illness severity, residual confounding mightiness beryllium present.
Although the planetary attack is considered a spot of PIFotal, and survey procedures were carried retired pursuing standardized protocols, the multi-country mounting whitethorn person introduced heterogeneity successful our data. Given our determination histrion (Fig. 2), it should beryllium acknowledged that matching the DPI to the patients’ needs should not beryllium solely based connected PIF, but that (among others) shared decision-making regarding inhalers17, prime of illness power and inhalation method are factors to consider5.
We supply objective recommendations for superior attraction clinicians to amended their attraction of COPD patients by limiting the imaginable antagonistic consequences of mismatching patients with inhalers. A important proportionality of COPD patients with insufficient inspiratory travel could payment from grooming targeting their highest inspiratory flow, oregon switching to an alternate DPI amended suited to the patient’s inspiratory ability, oregon progressive devices specified arsenic pMDIs oregon an SMI. Objective PIF measurements (against the absorption of the patient’s DPI), alternatively than inspiratory manoeuvre reflection ideally should usher the DPI enactment process successful superior care. HCPs should regularly measure the patient’s adherence, arsenic deliberate non-adherence was associated with debased PIF. Lastly, we concluded that HCPs should beryllium trained to amended the quality to place ‘critical’ inhalation method errors successful patients with COPD utilizing a DPI.
Data availability
The datasets generated during and/or analysed during the existent survey are disposable from the corresponding writer (JK) connected request.
References
Leving, M. et al. Impact of PIF, inhalation method and medicine adherence connected wellness presumption and exacerbations successful COPD: protocol of a real-world observational survey (PIFotal COPD Study). Pulm. Ther. 7, 591–606 (2021).
Kocks, J. W. H. et al. Factors associated with wellness presumption and exacerbations successful COPD attraction therapy with adust pulverization inhalers. NPJ Prim. Care Respir. Med. 32, 18 (2022).
Abdel-Aal, A. et al. Prioritising superior attraction respiratory probe needs: results from the 2020 International Primary Care Respiratory Group (IPCRG) planetary e-Delphi exercise. npj Prim. Care Respiratory Med. 32, 1–12 (2022).
Telko, M. J. & Hickey, A. J. Dry Powder inhaler formulation. Respir. Care 50, 1209–1227 (2005).
Peché, R., Attar‐zadeh, D., Scullion, J. & Kocks, J. Matching the Inhaler to the Patient successful COPD. J. Clin. Med. 10, 5683 (2021).
Loh, C. H., Peters, S. P., Lovings, T. M. & Ohar, J. A. Suboptimal inspiratory travel rates are associated with chronic obstructive pulmonary illness and all-cause readmissions. Ann. Am. Thorac. Soc. 14, 1305–1311 (2017).
van der Palen, J. Peak inspiratory £ow done Diskus and Turbuhaler, measured by means of a highest inspiratory £ow metre (In-Check DIAL s). Respir Med. 97, 285–289 (2003).
Sulaiman, I. et al. Objective Assessment of adherence to inhalers by patients with chronic obstructive pulmonary disease. Am. J. Respir. Critical Care Med. 195. https://doi.org/10.1164/rccm.201604-0733OC (2017).
Leving, M. et al. Suboptimal highest inspiratory travel and captious inhalation errors are associated with higher COPD-related healthcare costs. Int. J. Chron. Obstruct. Pulmon. Dis. 17, 2401–2415 (2022).
Chapman, K. R., Voshaar, T. H. & Virchow, J. C. Inhaler prime successful superior practice. Eur. Respiratory Rev. 14, 117–122 (2005).
Plaza, V. et al. Validation of the ‘Test of the Adherence to Inhalers’ (TAI) for asthma and COPD patients. J. Aerosol Med. Pulm. Drug Deliv. 29, 142–152 (2016).
Ställberg, B., Nokela, M., Ehrs, P. O., Hjemdal, P. & Jonsson, E. W. Validation of the objective COPD questionnaire (CCQ) successful superior care. Health Qual. Life Outcomes 7, 1–9 (2009).
Ghosh, S., Ohar, J. A. & Drummond, M. B. Peak inspiratory travel complaint successful chronic obstructive pulmonary disease: implications for adust pulverization inhalers. J. Aerosol Med. Pulm. Drug Deliv. 30, 381–387 (2017).
Price, D. B. et al. Inhaler errors successful the CRITIKAL study: type, frequency, and relation with asthma outcomes. J. Allergy Clin. Immunol. Pr. 5, 1071–1081.e9 (2017).
Leving, M. T., Kocks, J., Bosnic-Anticevich, S., Dekhuijzen, R. & Usmani, O. S. Relationship betwixt highest inspiratory travel and diligent and illness characteristics successful individuals with COPD—a systematic scoping review. Biomedicines 10, 458 (2022).
Basheti, I. A., Armour, C. L., Bosnic-Anticevich, S. Z. & Reddel, H. K. Evaluation of a caller acquisition strategy, including inhaler-based reminder labels, to amended asthma inhaler technique. Patient Educ. Couns. 72, 26–33 (2008).
Metting, E. I., van Dijk, L., El Messlaki, H., Luers, J. & Kock, J. Development of a shared decision-making instrumentality to enactment patients and their healthcare supplier successful choosing the champion inhaler device. Eur. Respiratory J. 52, OA1643 (2018).
Acknowledgements
The survey sponsor was the General Practitioners Research Institute; information postulation and investigation were performed by General Practitioners Research Institute. Boehringer Ingelheim was the backing and technological partner. The members of the PIFotal survey radical would similar to admit Dr. Jaco Voorham from Data to Insights Research Solutions for his assistance with the statistical analyses, Dr Wilma Zijlema for her assistance with the review, drafting and editing of the paper, and Dr. Hans Wouters for his publication to the task medication successful the archetypal signifier of the project. They would besides similar to convey each contributing researchers: Maria João Barbosa, Ana Margarida Cruz, Liliana Silva, Duarte Araújo, Eurico Silva, Daniel Castro, João Ramires, Ana Fernandes, Catarina Carvalho, Raquel Castro, Jerzy Zientek, Ewa Pasko, Witold Drzastwa, Tomasz Kachel, Kornelia Ciekalska, Krzysztof Wytrychowski, Bernard Panaszek, Krzysztof Kowal, Ebian Brill, Willemien Feenstra, Geert Struik, Hans Schuurman, Mariette van Oostrum, Hennie Holwerda Meekma, Boudewijn Dierick, George Amofa, Esther Kuipers, Lennard Ringnalda, Boris Tyndall, Mark Drenth, Peter Mast, Hilbert Talsma, Raoul Wolfs, Cobie Hoogeboom, Hanneke van Andel, Paul Stoutenberg, Nancy van de Laak, Tessa Hillaert, Laura Holtzer, Natascha Fehrmann, Anniek Makkinga – Maassen van den Brink, Annemarie Hilbink, Erik Feenstra, Murat Tek, Sabrina Burer, Jan van Ginkel, Rinze Boersma, Alyssa Bonger, Miguel Roman Rodriguez, Marina García Pardo, Alejandra Valero Suau, Laura López Velasco, Cecilia Amato, Francisco Palmer Simó, Alberto Abenza, Rosa Llull Vila, Bartolomé Llompart Van Belzen, Silvia Jimeno Martínez, Francesc Moranta Ribas, Margarita Perelló Oliver, Yolanda Gómez López, Patricia Ibañez Gómez, María Nieves Mendieta Lagos, Laura Bueno López, Virginia María Mirabal Sánchez, Ana Delia Rodríguez Delgado, Nils Fischer, Alicia González Sansó, Nayra Ramírez Mendoza, Valeria Gazzaneo, Paula Merced Guillama Rodríguez, Virginia Naranjo Guerrero, Jose Angel Suarez Caballero, Isidoro Souto Bethencourt, Juan R. Dominguez Beatell, Elena Vanesa Rojas Manrique, Maria Jose Sanz Orejas, Cary Perez Lorenzo, Jesús Antonio Pérez Jiménez, Silvia Lara Afonso Trujillo, Bartolomé Dominguez Del Río Boada, Stavroula Papageorgakopoulou, Eleytheria Vakouti, Claire Gkatzoudi, Thodoris Krasanakis, Dimitris Kounalakis, Izoldi Bouloukaki, Nikolaos Tsakountakis, Emmanouela Chronaki, Katherine Mary Borg and Kamila Abutalieva for their clip and efforts to execute the survey measurements and implicit diligent inclusion, adjacent successful the challenging times of the pandemic. Finally, they would similar to convey the participants who generously gave their clip to enactment successful the study.
Ethics declarations
Competing interests
M.T.L., J.v.C., L.D., I.v.d.H., Y.J., B.M., K.S., N.S. were employed by General Practitioners Research Institute (GPRI) astatine the clip of the study. In the past 3 years (2019–2021), GPRI conducted investigator- and sponsor-initiated probe funded by non-commercial organizations, world institutes, and pharmaceutical companies (including AstraZeneca, Boehringer Ingelheim, Chiesi, GSK, Mundipharma, Novartis, and Teva). S.B.-A. has received grants from TEVA, and idiosyncratic fees from TEVA, Boehringer Ingelheim, AstraZeneca, GSK, Sanofi and Mylan. J.C.d.S. reports oregon idiosyncratic fees from AstraZeneca, Bial, Boehringer Ingelheim, GSK, Medinfar, Mundipharma and Sanofi. B.C. received honorarium from GSK and Sanofi. R.D. has received grants and idiosyncratic fees from TEVA, Boehringer Ingelheim, AstraZeneca, GSK, Chiesi, Focus Care, and Glenmark. M.G.P. receives grants from AstraZeneca, GSK and Boehringer Ingelheim. A.G. and R.A.-E. are employees of Boehringer Ingelheim. R.G. has received idiosyncratic fees from AstraZeneca, GSK and Chiesi. F.L. received grants and idiosyncratic fees from GSK, idiosyncratic fees from AstraZeneca, Boehringer Ingelheim, Chiesi, Menarini International, Novartis, Orion, and Trudell International, extracurricular the submitted work. T.M. has nary competing interests to declare. J.M. received grants from Boehringer Ingelheim, during the behaviour of the study; and grants from AstraZeneca, Chiesi, Novartis, and GSK, extracurricular the submitted work. D.P. reports grants and idiosyncratic fees from AstraZeneca, Boehringer Ingelheim, Chiesi, Mylan, Novartis, Regeneron Pharmaceuticals, Sanofi Genzyme, Theravance and Zentiva (Sanofi Generics); grants from the British Lung Foundation, Respiratory Effectiveness Group, UK National Health Service, and AKL Research and Development Ltd; idiosyncratic fees from Cipla, GlaxoSmithKline, Kyorin, Merck, Mundipharma, Airway Vista Secretariat, EPG Communication Holdings Ltd, FIECON Ltd, Fieldwork International, OM Pharma SA, PeerVoice, Phadia AB, Spirosure Inc, Strategic North Limited, Synapse Research Management Partners S.L., Talos Health Solutions, and WebMD Global LLC; non-financial enactment from Efficacy and Mechanism Evaluation programme and Health Technology Assessment; stock/stock options from AKL Research and Development Ltd, which produces phytopharmaceuticals; owns 74% of the societal endeavor Optimum Patient Care Ltd (Australia and UK) and 92.61% of Observational and Pragmatic Research Institute Pte Ltd (Singapore); and 5% shareholding successful Timestamp, which develops adherence monitoring technology. M.R.-R. receives grants and idiosyncratic fees from AstraZeneca and GSK; and idiosyncratic fees from Boehringer Ingelheim, Chiesi, Menarini, Mundipharma, Novartis, Pfizer, TEVA and BIAL. I.T. reports grants and idiosyncratic fees from GSK, AstraZeneca, Boehringer Ingelheim, Menarini, Novartis, Chiesi and Elpen. OU reports grants and idiosyncratic fees from AstraZeneca, Boehringer Ingelheim, Edmond Pharma, Chiesi and GSK; grants from Edmond Pharma; and idiosyncratic fees from Napp, Mundipharma, Sandoz, Takeda, Cipla, COVIS, Novartis, Mereobiopharma, Orion, and Menarini. J.W.H.K. reports grants, idiosyncratic fees and non-financial enactment from AstraZeneca, GSK and Boehringer Ingelheim; grants and idiosyncratic fees from Chiesi Pharmaceuticals and TEVA; grants from Mundipharma; idiosyncratic fees from MSD and COVIS Pharma; and besides holds 72.5% of shares successful the General Practitioners Research Institute. IT is Editor-in-Chief of npj Primary Care Respiratory Medicine, and S.B.-A. and T.M. are Associate Editors. I.T., S.B.A., and TM were not progressive successful the journal’s reappraisal of, oregon decisions related to, this manuscript.
Additional information
Publisher’s note Springer Nature remains neutral with respect to jurisdictional claims successful published maps and organization affiliations.
Supplementary information
Rights and permissions
Open Access This nonfiction is licensed nether a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, organisation and reproduction successful immoderate mean oregon format, arsenic agelong arsenic you springiness due recognition to the archetypal author(s) and the source, supply a nexus to the Creative Commons license, and bespeak if changes were made. The images oregon different 3rd enactment worldly successful this nonfiction are included successful the article’s Creative Commons license, unless indicated different successful a recognition enactment to the material. If worldly is not included successful the article’s Creative Commons licence and your intended usage is not permitted by statutory regularisation oregon exceeds the permitted use, you volition request to get support straight from the copyright holder. To presumption a transcript of this license, sojourn http://creativecommons.org/licenses/by/4.0/.
About this article
Cite this article
Leving, M.T., Bosnic-Anticevich, S., van Cooten, J. et al. Clinical recommendations for adust pulverization inhaler usage successful the absorption of COPD successful superior care. npj Prim. Care Respir. Med. 32, 59 (2022). https://doi.org/10.1038/s41533-022-00318-3
Received: 16 August 2022
Accepted: 11 November 2022
Published: 27 December 2022
DOI: https://doi.org/10.1038/s41533-022-00318-3




 English (US)
English (US)